(11) You and your chief resident are the first responders to a code green (respiratory arrest) on the thoracic surgery ward. Amid the mayhem which follows, your chief resident tells you to perform an emergency surgical airway on the non-responsive patient while he looks for a code cart on another floor. Through which anatomic structure should the emergency surgical airway be inserted?
Explanation
Correct Answer:
Crico-thyroid membrane
Take-Home Message:
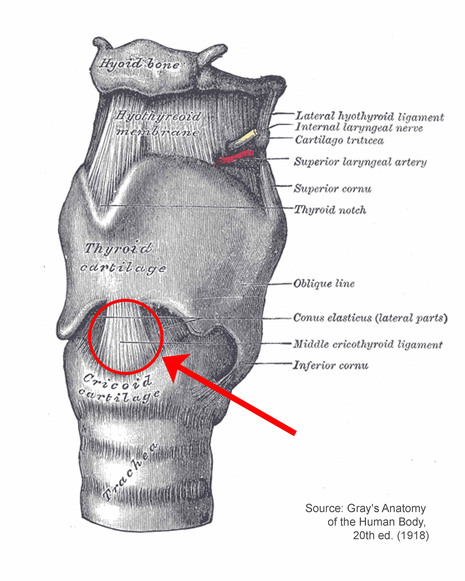
Emergency access to the airway can most safely be obtained by piercing the crico-thyroid membrane in the midline of the neck. This is termed a cricothyroidotomy.
Explanation of Correct Answer:
The cricoid cartilage is the only tracheal cartilage that is a complete ring. It is located immediately inferior to the wide,flat thyroid cartilage. There is generally a palpable indentation between the thyroid and cricoid cartilages, which represents the crico-thyroid membrane. These surface landmarks make this location an ideal one for performing emergency surgery to gain access to the airway. In the midline, there are no large crossing vessels and no important nerves.
Explanation of Incorrect Answers:
The hypopharynx is not an appropriate location for emergency airway access.
The thyroid cartilage is too hard to penetrate for placement of emergency airway access and might lead to laryngeal damage.
The cricoid cartilage is too hard to penetrate for placement of emergency airway access.
The tracheal rings limit the ability to place emergency airways.
Clinical Pearls:
If a patient needs prolonged respiratory support on a ventilator, a formal tracheostomy (or tracheotomy) procedure may be performed. This is different from the cricothyroidotomy outlined above in that the tracheostomy tube is placed through the tracheal rings below the cricoid cartilage. A tracheostomy is not a good emergency procedure because the thyroid is in front of the trachea and must be divided to place a tracheostomy.
For more information on this topic, please click on the following link(s):
(While these web sources have been vetted by our content experts, please use them with caution --- the peer-reviewed literature should be the ultimate source of medical information.)
Cricothyroidotomy. http://en.wikipedia.org/wiki/Cricothyroidotomy
Tracheotomy. http://en.wikipedia.org/wiki/Tracheostomy
Crico-thyroid membrane
Take-Home Message:
Emergency access to the airway can most safely be obtained by piercing the crico-thyroid membrane in the midline of the neck. This is termed a cricothyroidotomy.
Explanation of Correct Answer:
The cricoid cartilage is the only tracheal cartilage that is a complete ring. It is located immediately inferior to the wide,flat thyroid cartilage. There is generally a palpable indentation between the thyroid and cricoid cartilages, which represents the crico-thyroid membrane. These surface landmarks make this location an ideal one for performing emergency surgery to gain access to the airway. In the midline, there are no large crossing vessels and no important nerves.
Explanation of Incorrect Answers:
The hypopharynx is not an appropriate location for emergency airway access.
The thyroid cartilage is too hard to penetrate for placement of emergency airway access and might lead to laryngeal damage.
The cricoid cartilage is too hard to penetrate for placement of emergency airway access.
The tracheal rings limit the ability to place emergency airways.
Clinical Pearls:
If a patient needs prolonged respiratory support on a ventilator, a formal tracheostomy (or tracheotomy) procedure may be performed. This is different from the cricothyroidotomy outlined above in that the tracheostomy tube is placed through the tracheal rings below the cricoid cartilage. A tracheostomy is not a good emergency procedure because the thyroid is in front of the trachea and must be divided to place a tracheostomy.
For more information on this topic, please click on the following link(s):
(While these web sources have been vetted by our content experts, please use them with caution --- the peer-reviewed literature should be the ultimate source of medical information.)
Cricothyroidotomy. http://en.wikipedia.org/wiki/Cricothyroidotomy
Tracheotomy. http://en.wikipedia.org/wiki/Tracheostomy