Spinous Process of the Axis is the first bony point that can be felt in the midline inferior to the external occipital protuberance.
| Bone: Axis (anatomy) |
|---|
|
| Second cervical vertebra, or epistropheus, from above. |
|
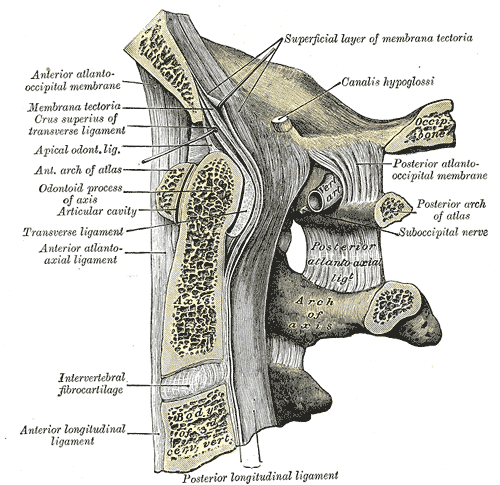
| Posterior atlantooccipital membrane and atlantoaxial ligament. (Axis visible at center.) |
| Gray's | subject #21 99 |
The Spinous process of the
vertebra prominens (C7) is easily palpable and is easily seen when the neck is flexed

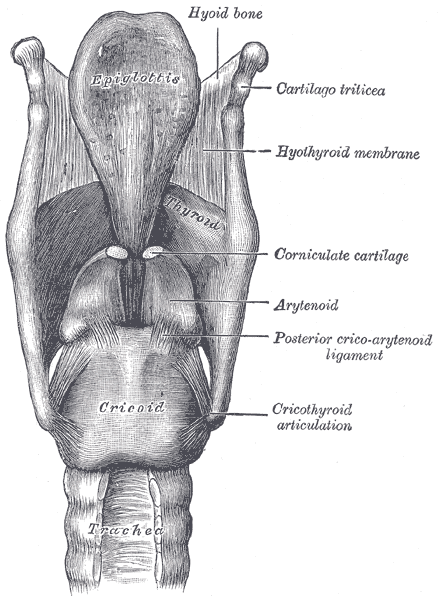
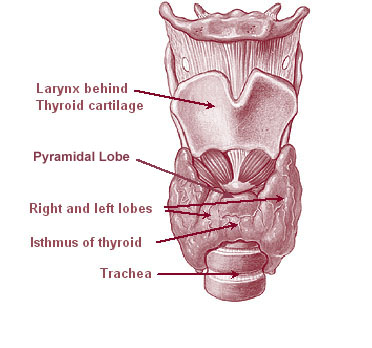
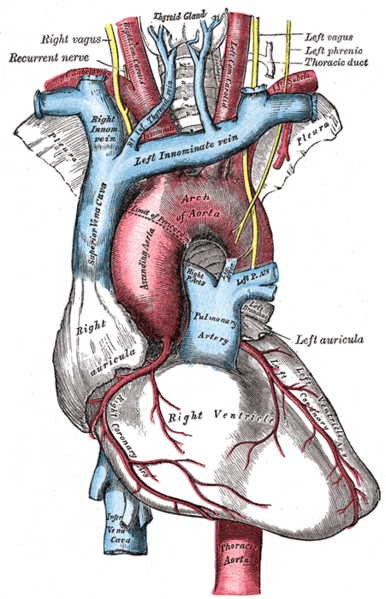
The Laryngeal prominence (Adam's Apple) formed by the thyroid cartilage. The sex difference in the angle formed by the laminae of the thyroid cartilage explains why the thyroid cartilage is more distinct in males.
Thyroid cartilage lies at the level of the 4th and 5th cervical vertebrae.
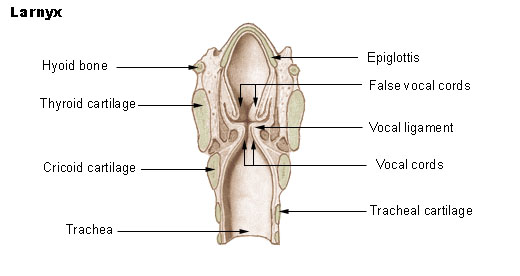





Vocal folds (true vocal cords) lie at the level of the midpoint of the anterior border of the thyroid cartilage
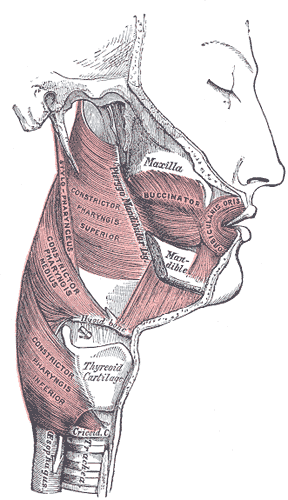
Hyoid Bone located at the level of the 3rd cervical vertibrae. The first resistant structure felt in the midline inferior to the chin - better felt when swallowing. The greater horn of the hyoid can be felt in relaxed patients fairly close to the anterior border of the sternocleidomastoid muscles.









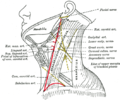
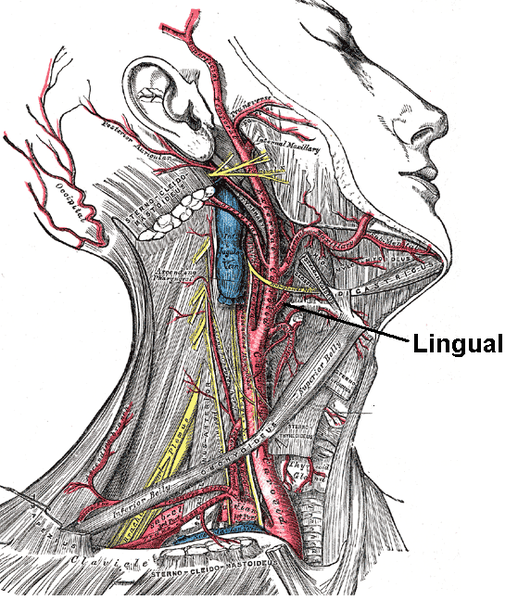
The tip of the greater horn of the hyoid bone lies midway between the laryngeal prominence and the mastoid process of the temporal bone - and forms an important landmark for locating the lingual artery posterior to the greater horn. Ligation of this artery is important when resecting the tongue for CA tongue.
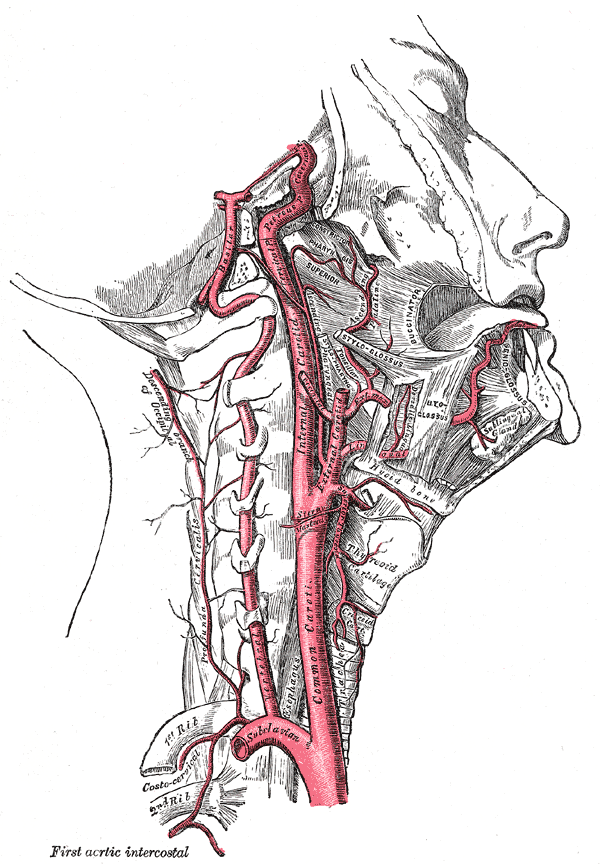
| Artery: Lingual artery |
|---|
|
| Superficial dissection of the right side of the neck, showing the carotid and subclavian arteries. The branch of the lingual artery is labeled |
|
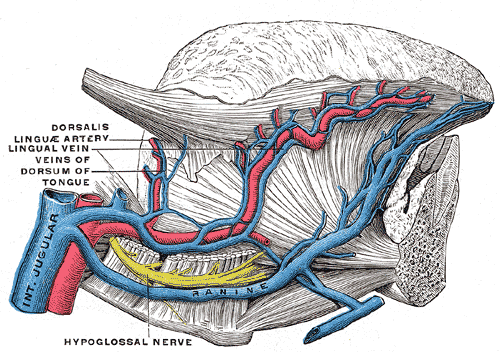
| Veins of the tongue. The hypoglossal nerve has been displaced downward in this preparation. (Lingual artery labeled at center left.) |
| Latin | arteria lingualis |
|---|
| Gray's | subject #144 553 |
|---|
| Supplies | genioglossus |
|---|
| Source | external carotid |
|---|
| Vein | lingual vein |
|---|

The tips of the transverse process of the atlas can be felt (C1) by deep palpation between the angle of the mandible and 1cm anteroinferior to the tip of the mastoid process.
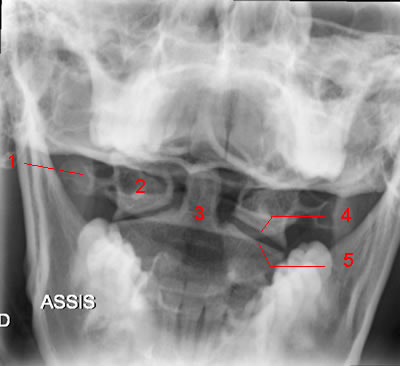 Atlas and odontoid process: AP view (Mouth wide open). 1, Transverse process of C1. 2, Lateral mass of C1. 3, Odontoid. 4, Inferior articular process of C1.5, Superior articular process of C2.
Atlas and odontoid process: AP view (Mouth wide open). 1, Transverse process of C1. 2, Lateral mass of C1. 3, Odontoid. 4, Inferior articular process of C1.5, Superior articular process of C2.
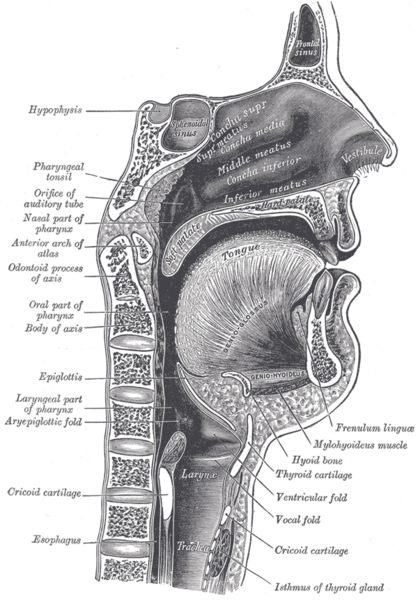
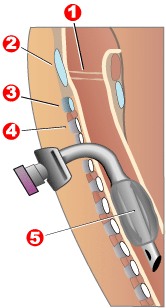
Cricoid cartilage
Important landmark in tracheotomy. level of the 6th cervical certebrae, when the pharynx joins the esophagus and the larynx and trachea. The tracheal rings are usually not palpable inferior to the cricoid cartilage, because the isthmus of the thyroid gland lies anterior to them.
Clinical significance
Anterior Cricoid Pressure was considered the standard of care during Rapid Sequence Intubation for many years.
[1] The American Heart Association still advocates the use of cricoid pressure during resuscitation using a
BVM, and during emergent oral endotracheal intubation.
[2] However, recent research increasingly suggests that cricoid pressure may not be as advantageous as once thought. The initial article by Sellick was based on a small sample size at a time when high tidal volumes, head-down positioning, and barbiturate anesthesia were the rule.
[3]Cricoid pressure may frequently be applied incorrectly.
[4] [5] [6] [7] [8] Cricoid pressure may frequently displace the esophagus laterally, instead of compressing it as described by Sellick.
[9] [10] Several studies demonstrate some degree of glottic compression
[11] [12] [13] reduction in tidal volume and increase in peak pressures.
[14]Based on the current literature, the widespread recommendation that cricoid pressure be applied during every rapid sequence intubation is quickly falling out of favor.
Gastric reflux could cause
aspiration if this is not done considering the general anesthesia can cause relaxation of the
gastroesophageal sphincter allowing stomach contents to ascend through the esophagus into the trachea.
A medical procedure known as a
cricoidectomy can be performed in which part or all of the cricoid cartilige is removed. This is commonly done to relive
blockageswithin the trachea.
[15]
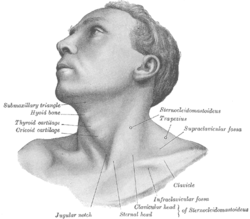
The Jugular Notch: Moves superiorly when swallowing. Jugular notch is palpable between the medial ends of the clavicle heads, and is clearly visible. It is the rounded depression in the superior border of the manubrium sterni. | Bone: Suprasternal notch |
|---|
|
| Suprasternal notch |
|
| Anterolateral view of head and neck. (Jugular notch labeled at bottom center.) |
| Latin | fossa jugularis sterni |
| Gray's | subject #27 120 |
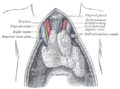
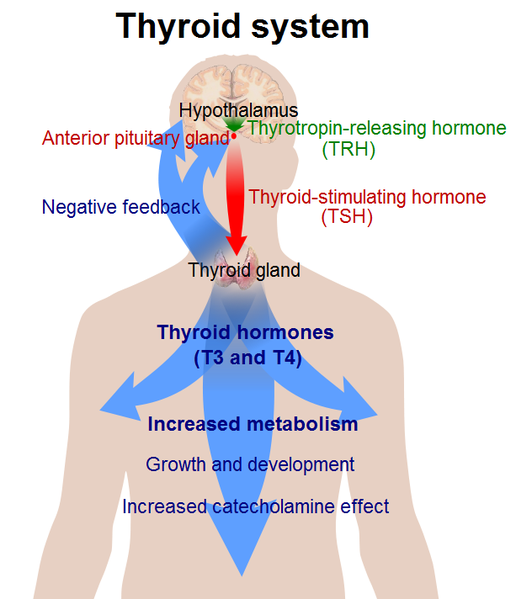
The lobes of the Thyroid may be palpable, particularly in females during menstruation and pregnancy. The lobes of the thyroid are connected in the midline - may be felt like a cushion like mass a finger breath inferior to the cricoid cartilage. The isthmus of the thyroid lies over the second and third tracheal rings

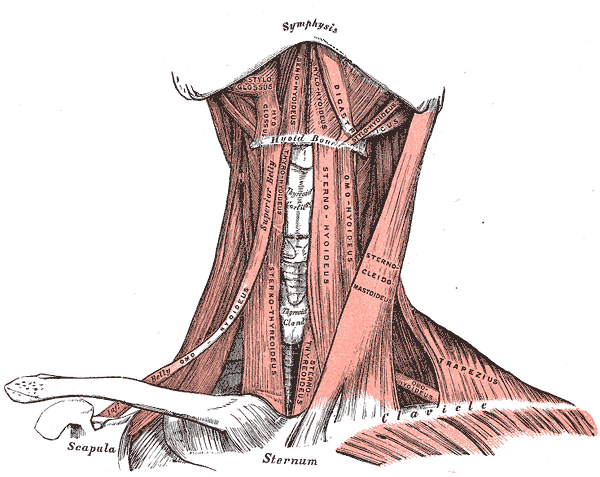



 The supraclavicular fossa lies between the tendinous sternal head and the clavicular head of the sternocleidomastoid muscle. This is a clinically significant because it contains the pressure point for the subclavian artery. In an emergency, the subclavian artery can be compressed in the supraclavicular triangle against the first rib preventing hemorrhage in the upper limb.
The supraclavicular fossa lies between the tendinous sternal head and the clavicular head of the sternocleidomastoid muscle. This is a clinically significant because it contains the pressure point for the subclavian artery. In an emergency, the subclavian artery can be compressed in the supraclavicular triangle against the first rib preventing hemorrhage in the upper limb. 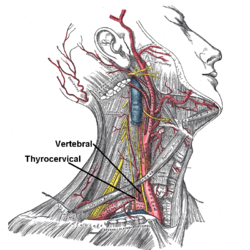
| Supraclavicular fossa |
|---|
 |
| Anterolateral view of head and neck. (Supraclavicular fossa labeled at center right.) |
 |
| Front view of neck. (Supraclavicular fossa labeled at center right.) |
| Latin | fossa supraclavicularis |
|---|